UKHSA guidance on the management of scabies cases and outbreaks in long-term care facilities and other closed settings
Updated 16 May 2024

© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/scabies-management-advice-for-health-professionals/ukhsa-guidance-on-the-management-of-scabies-cases-and-outbreaks-in-long-term-care-facilities-and-other-closed-settings
Executive summary
This national guidance has been developed to aid UK Health Security Agency (UKHSA) health protection teams (HPTs) and others involved in the management and control of scabies cases and outbreaks in long-term care facilities and other closed settings.
Previously, HPTs in England have developed and used local guidance which made variable recommendations (1).
The guidance is split broadly into 2 sections: management of single cases, and management of outbreaks. It is intended as a basis for consistent practice nationally, drawing upon the best available evidence and experience base.
Summary of public health management of cases and outbreaks of scabies in long-term care facilities and other closed settings
Management of single cases
Refer case to GP for treatment.
Identify close contacts (up to 8 weeks prior to diagnosis) including visitors.
Refer contacts for treatment.
Co-ordinate treatment of case and contacts to break cycle of transmission.
Provide hygiene and exclusion advice and avoid transfers to other settings during treatment.
Advise on appropriate personal protective equipment (PPE) for staff and visitors.
Management of outbreaks
If 2 or more linked cases within an 8 week period, assess all individuals (staff and residents) within the setting for scabies infection.
Identify close contacts (up to 8 weeks prior to diagnosis) including visitors.
Co-ordinate treatments of all cases and contacts linked to the setting.
Provide hygiene and exclusion advice and avoid transfers to other settings during treatment.
Advise on appropriate PPE for staff and visitors.
Consider isolation of residents or exclusion of staff until mass treatment completed.
Warn and inform visitors to setting until mass treatment completed.
This document should be used alongside other resources available including:
- Health protection in children and young people settings, including education (2022)
- Infection control in prisons and places of detention
- Care homes: infection prevention and control
- NICE clinical knowledge summaries: scabies (2022)
- Scabies: symptoms, diagnosis and treatment (BMJ Best Practice) (2022)
- British Association for Sexual Health (BASHH) and HIV UK national guideline on the management of scabies (2016)
Background
Scabies infection
Scabies is a skin condition caused by an immune reaction to the mite Sarcoptes scabiei and their saliva, eggs and faeces. The typical clinical presentation of infection is intense itching associated with burrows, nodules and redness. However, asymptomatic infection has been demonstrated in the elderly (2). Symptoms may last for weeks or months, can be hard to recognise and are often mistakenly attributed to other skin conditions, leading to avoidable transmission.
Scabies is most often transmitted by prolonged or frequent skin-to-skin contact. Itching may be severe, particularly at night and scratching may lead to secondary bacterial infection and its complications.
Crusted scabies, formerly known as Norwegian scabies, is a hyperinfestation where a much higher density (3) of mites is present, developing as a result of an insufficient immune response by the host.
Outbreaks of scabies are most likely to occur where people live in close proximity, and in settings where individuals receive personal or health care or staff working in these settings. The elderly, young (children and young adults) and immunocompromised are particularly vulnerable to scabies. Institutional settings such as care homes and prisons are especially susceptible to outbreaks (4).
Surveillance of scabies in England
The epidemiology of scabies in the UK is poorly understood and available disease surveillance data is limited. It is not a notifiable disease, and the majority of data comes from outbreaks reported to HPTs in England and reports from sexual health services via GUMCAD. Reports are predominantly from long-term care facilities; however, outbreaks are also reported in prisons, schools, and immigration detention centres.
Reliable estimates of scabies incidence are not possible, but it has been estimated that 1 in 50 long-term care facilities will experience an outbreak each year (4).
There is considerable stigma associated with scabies, which can contribute to under-reporting both in the community and among staff and residents in care facilities.
The role of the health protection team in scabies management
Scabies outbreaks can be challenging to manage due to difficulties in diagnosis (2) and in implementation of infection control and treatment measures required to break the chain of transmission. Although scabies is not a notifiable disease, due to these challenges UKHSA HPTs are able to support settings with the recognition and management of outbreaks.
The role of the HPT will vary depending on local arrangements. Broadly, the HPT can support settings and infection control teams by undertaking a risk assessment in conjunction with the setting manager or clinicians. The HPT can provide advice and support to the setting manager on the co-ordination of treatment, control measures and communications.
HPTs are not responsible for clinical diagnosis or prescribing of treatments, which ultimately lies with the NHS.
Management of single cases
Epidemiological parameters
Incubation period
Scabies is a skin infestation caused by the mite Sarcoptes scabiei. Scabies occurs when the mite burrows into skin and lay eggs that hatch into larva. The eggs hatch in 3 to 4 days and develop into adult mites in 1 to 2 weeks. Within the skin the adult female lays eggs and deposits waste products. Their presence in the skin usually causes itching, while the hatching of the eggs produces new larvae which can migrate to the surface of the skin and infect new hosts. In a first episode, symptoms are usually experienced within 3 to 6 weeks. People who have been re-exposed to scabies after successful treatment may develop symptoms more quickly, in around 1 to 4 days.
Period of infectiousness
Scabies is contagious from the point of infestation, that is, whenever mites are present on the skin.
Transmission route
Mites and larvae quickly desiccate and die outside their burrows. For this reason scabies is transmitted through close or prolonged skin contact with an affected person, for example, sharing a household setting, through the provision of intimate care, or via sexual contact. Transmission through casual contact such as a handshake is unlikely. The risk of transmission from cases of crusted scabies in close or prolonged skin contact is greater due to the greater number of mites present on the skin.
Fomite transmission
The importance of the role of fomites (for example, clothing, bed linen and towels) in scabies transmission is unclear and there is conflicting evidence in the literature (5, 6). Some evidence suggests that mites can live away from a host for up to 4 days; however, the likelihood of survival and successful infestation of a new host in that period is not known.
Zoonotic transmission
Animal scabies is caused by a different species of scabies mite than that found in humans. Transmission between humans and animals is not thought to occur in the UK. Animals with scabies (Sarcoptic mange) should be treated by a veterinarian.
Clinical presentation
Scabies
Scabies infection is primarily a clinical diagnosis made in the community.
‘Classical scabies’ refers to widely known typical presentation of lesions which are slightly raised with a linear burrow. The length can vary from a few millimetres to a centimetre. The mite can sometimes be seen at the leading edge as a black dot. In older children and adults, the burrows, nodules and rash are typically located in the webs of the fingers and toes, and on the sides of the hands and feet.
Lesions can also occur on the belt line, nipples, buttocks and genitals, although facial involvement is rare. Penile or scrotal nodules are highly specific for scabies. Children below the age of 5 can be affected from head to toe with eczematous lesions.
The first indications of a case of scabies include severe itching, usually most severe at night, and shallow burrows on the skin. This generally begins 3 to 6 weeks after infestation. A history of contact with a case, or reports of a persistent itch within a community setting, should raise suspicion.
Among elderly residents in long-term care settings, the clinical presentation may be very different. Burrows and rashes may affect parts of the body typically covered by clothing, for example, the torso or legs, therefore careful and thorough examination including the removal of clothing is recommended. Some may display no symptoms, especially in those with underlying cognitive impairment, and so diagnosis can be extremely challenging (2).
People with cognitive impairment may not be able to communicate that they are itching and may not scratch. Secondary infection with bacterial infection may mask an underling scabies infestation. Atypical presentations may occur in immunosuppressed patients.
Crusted scabies
Crusted scabies is a presentation which most commonly occurs in elderly, immunocompromised or malnourished people. This form of scabies is characterised by a scaly rash and thickened crusts of skin containing many mites, alongside heavy skin shedding. Itching may be absent. It is harder to treat and may contribute disproportionately to transmission.
Diagnosis
Currently available tests are rarely helpful in scabies diagnosis and management. The identification of burrows or mites with a dermatoscope is diagnostic of scabies but is not widely available in the community. The examination of skin scrapings with a light microscope to identify mites, mite eggs, or faeces is often considered to be the ‘gold standard’ but this method has poor sensitivity and is rarely performed (7).
Specialist dermatology services may be able to support in making a diagnosis of scabies but seeking this advice should not significantly delay commencing treatment or outbreak control measures, due to the distressing nature of symptoms and high likelihood of onward transmission in closed settings (2).
Single case management
For the clinical management of single cases of scabies please refer to the NICE guidance. Recommended treatment involves the application of permethrin (5%) cream (Lyclear), or malathion (0.5%) aqueous liquid (Derbac-M) if permethrin is not appropriate.
- Affected individuals can return to work, after completion of the first 24 hour treatment dose as prescribed by a clinician.
- Affected individuals should avoid close physical contact with other people until completion of the first 24 hour treatment dose.
- People with scabies should be advised that symptoms may persist for up to 6 weeks after treatment. Clinicians should consider prescribing antipruritics for the management of the itch if persistent or distressing.
- Where scabies has been acquired from a sexual partner a referral for and sexually transmitted infection (STI) screen should be advised.
- Staff and carers should wear appropriate PPE when handling and providing personal care until the first 24 hour treatment dose has been completed.
- Transfer of cases to other settings should be avoided until the first 24 hour treatment dose has been completed.
Management of contacts
Contacts are defined as anyone who has close physical contact with the case without appropriate PPE, for example, providing personal care with skin-to-skin contact, sharing a room or other similar household setting, and sexual partners, within the 8 weeks prior to diagnosis.
In the event of cases or outbreaks of crusted scabies, a higher index of suspicion of transmission via more transient contacts may be warranted. An individual case-by-case risk assessment is recommended to take into account severity of infection in the patient and any evidence of transmission without skin-to-skin contact, for example if a member of staff in contact with the patient environment but not with direct skin-on-skin contact is identified as a secondary case.
- Contacts should all be treated at the same time as the index case, on 2 occasions 7 days apart (even if asymptomatic). If staff contacts are off duty at the time of treatment, they should complete the first 24-hour treatment dose before returning to work.
- Have a low index of suspicion for identifying potential contacts of a case of crusted scabies due to the increased risk of transmission.
- Staff should be vigilant for signs and symptoms of scabies for an 8-week period and if 2 or more cases of scabies are identified in the setting then management should proceed as per an outbreak scenario.
- If the case has been transferred within 8 weeks of symptom onset from another setting, staff should inform management at that setting to investigate for possible close contacts and to consider implementing other control measures.
Laundry and environmental considerations
- All clothes, soft slippers, towels and bed linen of the affected case should be washed at a minimum of 50°C (122°F) on the day of application of the first treatment.
- If clothes cannot be washed at high temperature, they can be sealed in plastic bags for 4 days at room temperature, after which mites are unlikely to survive (5, 6).
- Alternative methods include pressing clothes with a warm iron, dry cleaning and putting items into a hot cycle in the dryer for 10 to 30 minutes.
- Appropriate PPE should be worn when handling any of these items.
- It is not necessary to fumigate living areas or furniture or treat pets.
See Appendix 2 for a factsheet that can be shared with cases or settings in the event of single cases.
Outbreak management in closed settings
Most outbreaks will occur within households. However, outbreaks also occur in residential settings including long-term care facilities, places of detention and boarding schools. The following section aims to provide guidance on the management of outbreaks in these settings where secondary case identification and breaking the cycle of transmission can be more challenging than in household settings.
A closed setting is therefore defined as any setting where a number of people are living with close contact inside the setting (shared bathroom or communal areas) and often more limited contact with the wider community, and includes the staff working within the setting.
Examples (not exhaustive) of closed settings include:
- care homes
- prisons
- long-term hotel or hostel accommodation
- homeless hostels
Definition of an outbreak in a closed setting
An outbreak is defined as 2 or more epidemiologically linked cases of scabies within an 8 week period.
Contact tracing
Before initiating treatment of single cases, all residents and staff should be checked for symptoms and signs of scabies. Assessing clinicians should be aware of the potential for asymptomatic infection, particularly in the elderly.
Contact tracing should identify contacts within the 8 weeks before the case’s diagnosis.
Contacts should be identified who meet the definition of a close contact.
These may include:
- all residents of the setting unless there is a clear rationale for more limited tracing (see below bullet points)
- residents on a single affected floor or wing if there is no mixing or movement of staff or residents and between floors or wings
- all members of staff (including agency staff) exposed to the index case without wearing appropriate PPE
- visitors to the setting who have had prolonged or frequent skin-to-skin contact with a case
- ancillary staff, for example, hairdressers, podiatrists, community health professionals and agency staff
It is recommended that all contacts receive treatment at the same time as cases. It is the responsibility of the setting or management team to ensure that this is coordinated as much as possible.
Co-ordination of mass treatment
All cases and contacts should be treated at the same time to break the cycle of transmission. If staff are off duty at the time of treatment, they should complete the first 24-hour treatment dose before returning to work. Individual case management should happen simultaneously for all cases and contacts in the outbreak.
Environmental measures are generally taken to reduce the potential risk of fomite transmission and reinfection. The evidence for a single optimal approach to environmental management is limited (8).
A number of studies describe challenges to the co-ordinated approach to an outbreak (1). Here we describe an approach found to be feasible in the experience of contributing HPTs.
Where occupational exposure of staff has led to their need for treatment, it is recommended that the employer should consider funding any treatment rather than staff paying for their own prescriptions. This encourages treatment uptake and promotes a prompt return to normal working. Social care settings can consider discussing alternative funding options with local authority public health or social care commissioning teams.
Ivermectin is a recognised off-label single- or double-dose oral treatment for scabies within closed settings, when there are logistical considerations in the successful delivery of topical therapy, or in the context of immunosuppression or crusted scabies (9). The decision to prescribe ivermectin in this context lies with local specialist dermatology and infectious diseases services.
Exclusion or isolation of cases in closed settings
Classical scabies
Isolation of residents who are diagnosed as having scabies is not usually warranted in the event of an outbreak, as once an outbreak has been identified contacts will either be wearing appropriate PPE or undergoing treatment at the same time.
Close contact with persons not undergoing concurrent treatment or unable to wear appropriate PPE should be limited as much as possible, for example, for patients who may find treatment challenging or distressing, such as people experiencing dementia or living with learning difficulties.
If uncertain that a treatment has been completed successfully (for example, rubbing off of cream prematurely, or inability to provide full cream coverage), consult specialist clinical advice from dermatology services on alternative treatments such as oral ivermectin.
Crusted scabies
Crusted scabies is highly transmissible; however, standard infection control principles and wearing appropriate PPE to avoid skin-to-skin contact should be sufficient to prevent transmission. Isolation of people with crusted scabies is therefore not recommended. Close contact with persons not undergoing concurrent treatment or unable to wear appropriate PPE should be limited as much as possible.
Affected individuals may require several applications of treatment or oral ivermectin in order to fully treat infection. Due to the complexities of treating crusted scabies, the decision as to whether the patient is no longer infectious should be guided by the specialist clinician involved in care. Limiting skin-to-skin contact where possible is advisable until non-infectious.
Staff
Members of staff who are diagnosed as having scabies, or identified as contacts of a case, should not return to work (in the affected setting or others they may work in) until after their first 24-hour treatment dose is completed. They should co-ordinate their treatment doses to coincide with the care home’s treatment dates.
Staff members identified as cases who have household or other contacts identified in the community should advise their contacts to also co-ordinate their treatment doses as much as possible, to avoid further transmission back to that staff member.
It is the responsibility of the setting management team to determine the most appropriate route for staff to access treatment, for example, through occupational health services, setting healthcare teams or GPs, or their own personal GPs.
Any agency staff diagnosed with scabies should inform their other places of work including home (domiciliary) care recipients so that these settings can also be risk assessed and clients identified.
Control measures
PPE
Standard infection control principles should be sufficient to prevent transmission. For most activities, gloves and plastic aprons are appropriate. However, for activities such as close personal care and handling where skin contact with patient skin, infested linen or clothing could occur, single patient use long sleeve gowns or sleeve protectors may be beneficial to reduce the risk of transmission.
Environmental management
Cleaning
The aim of cleaning in the event of a case or outbreak of scabies is to remove skin scales and dust in the environment. The role of fomites in transmission of scabies is unclear; however, mites are very unlikely to survive without a host long enough to infest a new person.
For classical scabies cases and outbreaks, the normal cleaning regimen will therefore be sufficient to remove skin scales from the environment. For crusted scabies, more regular vacuuming and a deep clean after treatment cycles (for example, damp dusting soft furnishings, cleaning touch points, vacuuming mattresses and so on) should be considered due to the increased shedding of skin associated with this form of scabies.
Laundry
Settings should already be compliant with guidelines around decontamination of laundry such as (HTM 01-04) Decontamination of linen for health and social care.
Residents’ clothing
Clothing which has been worn by affected individuals in the period prior to completion of the first 24 hour treatment dose should be handled using appropriate PPE. It is recommended to collect these items in a dissolvable alginate bag (soluble laundry bag), which is placed without opening into a compatible washing machine where available.
The contaminated items should not be mixed with those belonging to unaffected residents.
If residents’ clothing will not be able to withstand an infected linen process, it is acceptable to process these items separately in a hot wash (minimum 50°C (122°F)). Do not place in a mixed wash with clothing from other residents or overload the machine. The wash should be followed by tumble drying on a hot cycle for at least 10 minutes.
Any items which cannot be laundered in a hot wash may be placed in a sealed plastic bag for at least 4 days prior to laundering: this should be sufficient to kill any mites present. It should not be necessary to launder any items that have not been touched by the resident in the past week.
Linen and towels
Bed linen and towels of cases should be processed as infected linen. Items should be placed in dissolvable alginate bags (where available and if compatible with available washing machines) and either processed in a commercial or the on-site laundry using an enhanced process:
- wash temperature should be at least 50°C (122°F)
- thermal disinfection at 71°C for 3 minutes or 65°C for 10 minutes is advised
- linen should not be removed from water-soluble bags or sorted by hand
- washing machines should not be overloaded
- after laundering items should be dried immediately in a tumble drier
Family and visitors
Family members and other regular visitors (for example, healthcare staff, hairdressers and podiatrists) to the setting who may or may not have close physical contact with cases should be advised about the scabies outbreak, be given advice on the symptoms of scabies and advised where appropriate to seek treatment from their GP if they meet the definition of a case or contact. See Appendix 2 for a leaflet addressing common questions.
It is recommended that a notice is made visible in a public area to inform visitors that an outbreak of infection is currently being experienced and advise on wearing of appropriate PPE for any close contact.
All visits to the setting and individuals should be risk assessed appropriately. The benefits of visits to residents are likely to greatly outweigh the risks to visitors, which can be managed by recommending avoiding skin-to-skin contact and wearing of appropriate PPE
Essential visits and transfers, healthcare workers and health care settings
Visiting healthcare workers (for example, district nurses or physiotherapists) who have close or prolonged physical contact with residents should be informed of the outbreak prior to their visit to setting and reminded of the importance of wearing appropriate PPE for any skin contact with affected residents.
Transfers out of the setting experiencing an outbreak
If a case or contact requires transfer to a new closed setting (for example, hospital or care home), the admitting setting should be informed of the outbreak prior to the admission and a risk assessment undertaken. Transfers of cases and contacts should ideally occur after the first 24 hour treatment dose, at which point the risk of onward transmission is minimal. Transfers can take place sooner than this if appropriate mitigations are agreed. The risk assessment should consider at least:
- whether the person requiring transfer has completed the initial 24 hour treatment dose and whether transfer can be delayed until this has taken place
- whether close, prolonged skin-to-skin contact with others can be avoided during the treatment period, for example, whether the person is prone to walking with purpose or hand holding
- whether staff caring for the patient are able to maintain use of appropriate PPE during close contact until the treatment period has ended
People who do not meet the definition of case or contact can be transferred as usual.
Accepting new transfers during an outbreak
Management should consider and discuss with their social care commissioners, community infection control or local HPT the need to temporarily close admissions in the event of a scabies outbreak until the full course of treatment is completed or the outbreak is declared over.
New admissions to settings experiencing a scabies outbreak may be possible with appropriate risk assessments, which should include:
- how new admissions can be separated from affected individuals or staff
- whether new admissions have any pre-existing conditions that may make them more vulnerable to scabies infection or at risk of more severe sequelae
- whether admissions can be delayed until at least the first 24-hour treatment has been completed by all cases and contacts
- whether the outbreak is proving challenging to control, for example, difficulties in co-ordinating mass treatment, which may increase risk to others entering the setting
Declaring the outbreak over
For the purposes of reporting and determining provision of ongoing support, an outbreak can be considered over when all cases and contacts have received the full recommended treatment regimen (for example, 2 doses of topical cream application). However, ongoing monitoring and a period of heightened surveillance after all cases and contacts have completed treatment is advised to reduce the risk of outbreaks continuing unchecked.
This period of heightened surveillance should include regular re-assessment of staff and residents for any new symptoms, and to ensure symptoms are resolving as expected following treatment, and should last for 12 weeks (that is, 2 mite incubation cycles) after the onset date of symptoms in the last known case.
A scabies outbreak can be declared over if no new cases are identified within 12 weeks of symptom onset date of the last known case. Nodules can take several months to resolve after successful treatment.
Recurrent infections and outbreaks
It is important to note that symptoms (that is, itch or rash) may continue for up to 6 weeks after treatment completion, and does not necessarily imply a failure of treatment or re-infestation. It is recommended that resident or staff members who remain symptomatic after treatment are reviewed by their GP to rule out other possible causes of their symptoms and provide symptomatic relief for itching.
If further scabies outbreaks occur within 12 weeks of the original outbreak this should be flagged to the HPT and relevant infection prevention and control teams to review whether this is a new outbreak or a continuation of the original outbreak. In both scenarios, infection control procedures and treatment regimens should be reviewed carefully to identify possible failures in breaking the transmission chain or de-infestation.
Summary flowchart
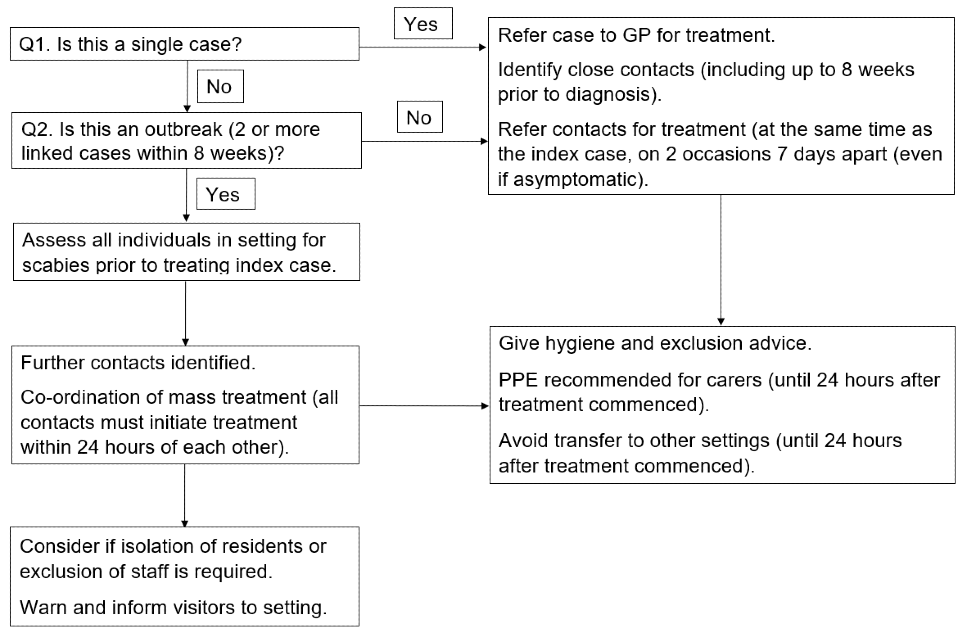
Accessible text version of summary flowchart
Question 1. Is this a single case?
If yes:
- refer case to GP for treatment
- identify close contacts (including up to 8 weeks prior to diagnosis)
- refer contacts for treatment (at the same time as the index case, on 2 occasions 7 days apart (even if asymptomatic)
If no, go to question 2.
Question 2. Is this an outbreak (2 or more linked cases within 8 weeks)?
If no, go to the 3 steps listed above.
If yes, assess all individuals in setting for scabies prior to treating index case.
Then, further contacts must be identified, with the co-ordination of mass treatment (all contacts must initiate treatment within 24 hours of each other).
Then take the following steps:
- give hygiene and exclusion advice
- PPE recommended for carers (until 24 hours after treatment commenced)
- avoid transfer to other settings (until 24 hours after treatment commenced)
- investigate possible chain of transmission or liaise with other relevant settings
Lastly:
- consider if isolation of residents or exclusion of staff is required
- warn and inform visitors to setting
End of flowchart text.
Appendix 1. Scabies Guidance Working Group membership
The Scabies Guidance Working Group met periodically, in person and virtually, between 2018 and 2021. Its membership consisted of clinicians, academics, experts by experience (for example, care home managers) and public health specialists with an interest in the management of scabies cases and outbreaks. The members were:
- Emily Phipps, Consultant in Communicable Disease Control, UKHSA South East
- William Welfare, Consultant in Health Protection, UKHSA North West
- Ellie Maslen, Senior Health Protection Practitioner, UKHSA London
- Karen Hawker, Senior Health Protection Practitioner, UKHSA London
- Mary Maimo, Senior Health Protection Practitioner, UKHSA London
- Jill Hendey, Health Protection Practitioner, UKHSA South East
- Judith Rushby, Health Protection Practitioner, UKHSA Yorkshire and Humber
- Jayshree Dave, Consultant Microbiologist, formerly of Public Health England (PHE) Public Health Laboratory for London
- Stefania Lanza, Research Co-ordinator, Brighton University Medical School
- Helen Fabrizio, Deputy Lead Nurse, Manchester City Council
- Stephen Walker, Consutlant Dermatologist, Hospital for Tropical Diseases, University College London Hospitals NHS Foundation Trust and Associate Professor, London School of Hygiene and Tropical Medicine
- Jackie Cassell, Honorary Consultant in Primary Care Epidemiology, Deputy Head of School Brighton and Sussex Medical School
- Jo Middleton, Research Fellow, Brighton and Sussex Medical School
- Melanie Berry, Health Protection Practitioner, UKHSA North West
- Joy Fletcher, Public Advisor
- Christopher Harland, Consultant Dermatologist, Epsom and St Helier University Hospitals NHS Trust
- Stephen Minto, Health Protection Practitioner, UKHSA North East
- Dr Anath Nalabanda, General Practitioner
- Selina Rajan, Public Health Registrar, UKHSA South East
- Pavlina Petrova, Principal Health Protection Practitioner, UKHSA South East
- Maaike Pietzsch, Senior Health Protection Practitioner, UKHSA South East
- Dr Jessica Banks, Public Health Speciality Registrar, UKHSA South East
- Ann Lusmore, Senior Health Protection Nurse, UKHSA London
The preparation and publication of this guidance was supported by the Regions Programmed Delivery Unit.
Appendix 2. Scabies information sheet
Scabies explained
Sarcoptes scabei is a human mite which penetrates the outer layers of the skin. The body’s immune system reacts to the mite’s droppings and saliva resulting in an immune reaction, which produces an intense itching.
The incubation period is up to 8 weeks after contact with an affected person. Skin penetration is visible as papules, vesicles or tiny linear burrows containing the mites and their eggs. The lesions occur mainly on the hands, finger webs, wrists and inside of arms, abdomen or waist, groin and under buttocks. In infants, the head, neck, palms and soles may be involved; these areas are often spared in older individuals.
The intense itch is aggravated by warmth and moistness. Itching occurs especially at night or after a hot bath or shower. Because of scratching, lesions can develop a secondary infection.
How scabies is spread
The mite is transferred to other people by prolonged, direct skin-to-skin contact, especially via the hands. It can also be acquired during sexual contact. Transfer from underclothes or bed linen may occur if these items have been contaminated by an affected person immediately before contact; mites do not survive away from their host, as it is too cold for them outside the skin. An individual is infectious until after effective treatment and should be kept away from work or school until this has been completed.
How scabies is treated
A scabies infection will not resolve without treatment. Insecticide creams or lotions are used to treat scabies, which are available through your GP. The following principles should be followed:
- Apply the cream over the whole body onto clean, cool, dry skin, but not directly after a bath.
- Ensure the cream is put under the nails, on the skin of the face, scalp, behind the ears, the soles of feet and on the genitals regardless of manufacturer’s instructions taking care to avoid eyes, nose and mouth.
- Directly after treatment, put on clean clothes and change the bed linen.
- Leave the cream on for 8 to 12 hours (overnight treatment will ensure this).
- If you wash your hands within 8 to 12 hours, reapply the cream to the hands making sure to put cream under the nails. Re-treat after one week.
- All bed partners and close family contacts should also be treated as above.
- Machine wash (at 50ºC (122ºF) or above) clothes, towels and bed linen on the day of application of the first treatment.
- If someone has crusted scabies, it is important to thoroughly clean the affected person’s environment to remove any skin scales in dust. This includes vacuuming carpets and furniture, washing bedding, clothes, curtains and cushion covers. Keep any items of clothing that cannot be washed in plastic bags for at least 4 days to contain the mites until they die. Pressing clothes with a warm iron, dry cleaning and putting items in a dryer on the hot cycle for 10 to 30 minutes is also effective.
After treatment it may take up to 6 weeks for the itching to stop, but this does not mean treatment has failed. Itching is a result of an allergic reaction to the mites. Antihistamines may help to relieve the itching.
Further information is available from NHS Choices.
References
1. White LCJ, Lanza S, Middleton J, Hewitt K, Freire-Moran L, Edge C and others. ‘The management of scabies outbreaks in residential care facilities for the elderly in England: a review of current health protection guidelines. Epidemiology and Infection 2016: volume 144, issue 15, pages 3,121 to 3,130. doi: 10.1017/S0950268816001746
2. Cassell JA, Middleton J, Nalabanda A, Lanza S, Head MG, Bostock J, Hewitt K, Jones CI, Darley C, Karir S, Walker SL. ‘Scabies outbreaks in 10 care homes for elderly people: a prospective study of clinical features, epidemiology, and treatment outcomes.’ The Lancet Infectious Diseases 2018: volume 18, issue 8, pages 894 to 902. doi.org/10.1016/S1473-3099(18)303OLD ^47-5
3. Bernigaud C, Fischer K, Chosidow O. ‘The management of scabies in the 21st century: past, advances and potentials.’ Acta Dermato-Venereologica 2020: volume 100, issue 9: :adv00112. doi:10.2340/00015555-3468
4. Hewitt KA, Nalabanda A, Cassell JA. ‘Scabies outbreaks in residential care homes: factors associated with late recognition, burden and impact. A mixed methods study in England.’ Epidemiology and Infection May 2015: volume 143, issue 7, pages 1,542 to 1,551. doi: 10.1017/S0950268814002143
5. Pallesen K, Lassen JA, Munk NT, Hartmeyer GN, Hvid L, Bygum A. ‘In vitro survival of scabies mites.’ Clinical and Experimental Dermatology 2020: volume 45, issue 6, pages 712 to 715.doi: 10.1111/ced.14209
6. Bernigaud C, Fernando DD, Lu H, Taylor S, Hartel G, Chosidow O, Fischer K. ‘How to eliminate scabies parasites from fomites: a high-throughput ex vivo experimental study.’ Journal of the American Academy of Dermatology 2019: volume 83, issue 1, pages 241 to 245. doi.10.1016/j.jaad.2019.11.069
7. Walton SF, Currie BJ. ‘Problems in diagnosing scabies, a global disease in human and animal populations.’ Clinical Microbiology Reviews 2007: volume 20, issue 2), pages 268 to 279 doi: 10.1128/CMR.00042-06
8. Morrison, E J, Middleton, J, Lanza, S, Cowen, J E, Hewitt, K, Walker, S L, Nicholls, M, Rajan-Iyer, J, Fletcher, J and Cassell, J. ‘Do we know how scabies outbreaks in residential and nursing care homes for the elderly should be managed? A systematic review of interventions using a novel approach to assess evidence quality.’ Epidemiology and Infection 2019: volume 147, page e250. doi:10.1017/S0950268819001249
9. Middleton J, Walker SL, House T, Head MG, Cassel JA. ‘Ivermectin for the control of scabies outbreaks in the UK.’ Lancet 2019: volume 394, issue 10,214, pages 2,068 to 2,069. doi:10.1016/S0140-6736(19)32619-4